

How To Repair An Ac Joint
Original Editors - Mathilde De Dobbeleer - Killian Borms, Haytem Mkichri, Anna Jansma, Yassin Khomsi. equally office of the Vrije Universiteit Brussel Evidence-Based Practice Project Height Contributors - Mostafa Mataich, Kim Jackson, Mathilde De Dobbeleer, Scott Cornish, Ilona Malkauskaite, Lien Hennebel, Admin, Yuli-Karisma Borremans, Rachael Lowe, WikiSysop, Fasuba Ayobami, Simisola Ajeyalemi, Vidya Acharya, Borms Killian, Wanda van Niekerk, Venus Pagare, George Prudden, Kai A. Sigel, Tony Lowe, Oyemi Sillo, Amanda Ager, Naomi O'Reilly, Lucinda hampton, Olajumoke Ogunleye and Tarina van der Stockt
Definition/Clarification [edit | edit source]
Disorders is a general term to comprehend a range of conditions. It can be due to trauma, such as joint dislocation of the acromioclavicular joint or degenerative atmospheric condition, such as osteoarthritis.[one] An acromioclavicular dislocation is a traumatic dislocation of the articulation in which a displacement of the clavicle occurs relative to the shoulder.[two]
Clinically Relevant Anatomy [edit | edit source]
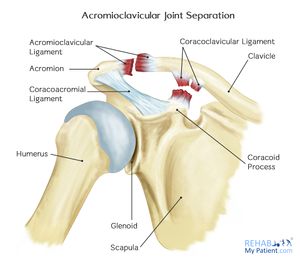
The acromioclavicular joint is a diarthrodial articulation with an interposed fibrocartilagninous meniscal disc that connects the clavicle with the acromion. It has an intra-articular synovium and an articular cartilage interface[3] and is characterised by the diverse angles of inclination in the sagittal and coronal planes and by a disc. 2 types of disc have been observed; a consummate disc (very rare) and a meniscoid-like disc. [iv].[5] The acromioclavicular joint is surrounded by a capsule and reinforced by the superior/inferior capsular ligaments with the coracoclavicular ligaments (trapezoid and conoid) likewise important structures for stability of the joint.[6]
The acromioclavicular (Air conditioning) ligament and coracoclavicular (CC) ligaments are function of the static stabilisers of the joint. The Air-conditioning ligament controls horizontal stability in the anteriorposterior airplane whilst the CC ligaments serve to control vertical stability. The conoid part of this ligament attaches posteriorly and medially on the clavicle with the trapezoid office attaches anteriorly and laterally. The trapezius and deltoid muscles also provide dynamic stabilisation of the AC articulation.[7]
Epidemiology /Etiology [edit | edit source]
Injuries to the AC Joint account for approximately 10% of acute injuries to the shoulder girdle, with separations of the AC Joint accounting for xl% of shoulder girdle injuries in athletes. Normally, injury happens when falling onto an outstretched hand or elbow, direct blows to the shoulder, or falling onto the point of the shoulder.[6]
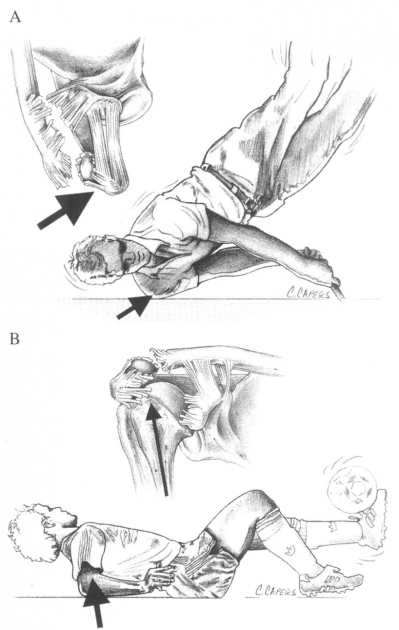
Figure 2 illustrates the common mechanism of injury:
(A) a direct forcefulness onto the point of the shoulder
(B) indirect forces to the AC joint can too crusade injury. For case, a fall on to the elbow can drive the humerus proximally, disrupting the AC joint. In this instance, the force is referred only to the Air conditioning ligaments and not the coracoclavicular ligaments.[8]
The injury is frequently seen in hockey and rugby players, but is besides seen in alpine skiing, snowboarding, football game, cycling and motor vehicle accidents. [9] [ten]
Characteristics/Clinical Presentation [edit | edit source]
With an AC articulation injury pain is often felt radiating to the neck and deltoid. The AC joint may too go swollen, the upper extremity oftentimes held in adduction with the acromion depressed, which may crusade the clavicle to be elevated.[11]
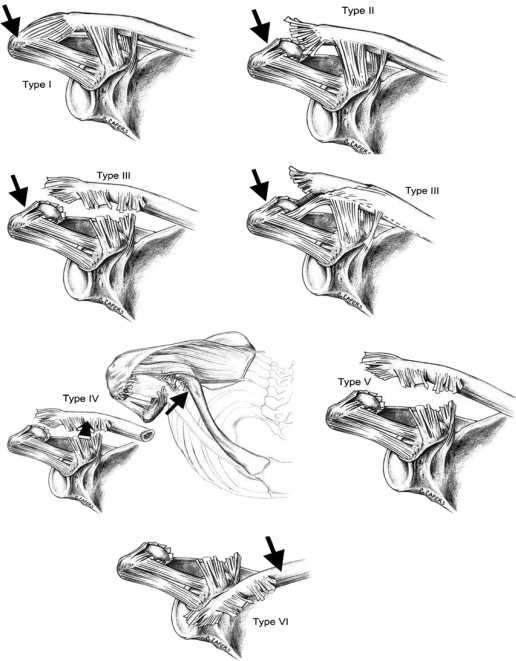
Allman et al described a 3 grade classification with Rockwood and Greenish expanding this to a 6 course classification model (known as the Rockwood grades). This classification of Air-conditioning joint injuries assists in deciding on appropriate treatment options and helps to avoid complications past failure to recognise the pattern of injury. [12]
| Course | Description | Ascertainment/Testing |
|---|---|---|
| I | Sprain of AC ligaments. The AC and CC ligaments are intact | No instability of clavicle detected on stress tests |
| 2 | AC ligaments are ruptured, CC ligaments are intact. Often described as a subluxation. | Clavicle is unstable to direct stress tests |
| III | Complete disruption of both the Air conditioning and CC ligaments without pregnant disruption of the delto-trapezial fascia. This is oftentimes described as a dislocation. | Deformity present with clavicle actualization elevated (acromion depressed), clavicle unstable in both vertical and horizontal airplane |
| Four | Distal clavicle is posteriorly displaced into trapezius muscle | Posterior deformity present. |
| V | More severe grade of grade III. Complete disruption of both the AC and CC ligaments with disruption of the delto- trapezial fascia. | Pseudo lateral clavicle summit, downward displacement of the scapular. |
| VI | Inferior displacement of the distal clavicle, either subacrominal or subcoracoid | Severe trauma, commonly accompanied by other pregnant injuries. |
Using digital measurement instead of a solely visual diagnosis is recommended because of the higher intra- and interobserver reliability.[thirteen]
Differential Diagnosis [edit | edit source]
- Most dislocations are situated in the Glenohumeral joint and 90% of this dislocations are anterior which tin can cause concomitant pathologies such as a Hill sachs lesion or injury of the brachial plexus. [14]
- Pain in the Ac joint from osteoarthritis or disc illness[15]
- Osteolysis of the distal clavicle [xvi]
- Instability of the AC articulation[16]
- Rotator-cuff impingement or tear[16]
- Adhesive capsulitis[16]
- Thoracic outlet syndrome[16]
- Superior labral tears[16]
- Complex pain syndrome[16]
- Shoulder dislocation [six]
- Anterior humerus subluxation [6]
Diagnostic Procedures [edit | edit source]
- Acromioclavicular dislocation is oftentimes diagnosed via radiography. Possible problems can occur with patients suffering from a blazon I injury equally nothing aberrant is evident on a radiograph. Diagnosis is therefore determined past the mechanism of injury and tenderness over the Air-conditioning joint.[17]
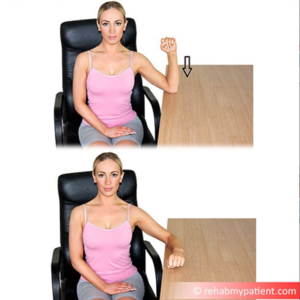
- Resisted AC Articulation Extension Test
Issue Measures [edit | edit source]
- Dash: Disabilities of the Arm, Shoulder and Hand questionnaires.[12]
- Simple Shoulder Test questionnaires: Purpose is to assess functional disability of the shoulder, scored from 12 questions: 2 nearly part related to pain, 7 nearly function/strength and 3 nigh range of move [12]
- Shoulder Pain and Disability Index (SPADI): The primary result measure is the patients' perceived level of pain and disability. Information technology consists of 2 subscales, pain and disability, which are combined to produce a total score ranging from 0 (no hurting or functional difficulty) to 100 (highest level of pain and functional difficulty). The SPADI is reliable, valid, and responsive for shoulder hurting of musculoskeletal, neurogenic, or undetermined origin. [xviii]
- American Shoulder Elbow Surgeon (ASES): This measures functional limitations and pain in patients with musculoskeletal shoulder pathologies. The functional score is calculated from 10 questions relating to function using a 4 point scale.[18]
Test [edit | edit source]
- Ac Joint Palpation for Tenderness
- O'brien test: Examination using the O'Brien exam tightens the posterior sheathing and posteriorly translates the humeral caput, stressing the labrum resulting in pain and weakness.
- Paxinos sign: Provocative testing for acromioclavicualr joint injury[eleven] [19]. Walton et al found that the Paxinos examination is a good clinical diagnostic tool and bone scanning is the most reliable imaging modality for the diagnosis of Air-conditioning articulation pathology. When both of these tests are positive, there is a high degree of confidence for a diagnosis of AC joint pathology [19].
- Test of Stenvers 4: Clavicular Roll
- Resisted Air-conditioning Joint Extension Test
A history of the mechanism of injury and palpation of the AC joint help to differentiate between a type I and a type II injury. A modest deformity in the AC articulation is indicative of a type 2 injury. In a type I injury, swelling is usually nowadays with pain on abduction of the arm, whereas with a type II pain is unremarkably experienced in all movements of the arm. An obvious footstep deformity of the AC articulation indicates a type Iii injury and the patient commonly supports the injured arm as close as possible to his trunk.[twenty]
[21]
Medical Management [edit | edit source]
Treating an AC joint injury will vary depending on its severity.
Nonoperative treatment is recommended for type I and type II Air-conditioning separations, but for blazon Iii this is nonetheless much debated, as there is a high take a chance of early onset degenerative within the joint. However surgical intervention may be chosen as in sure cases this may yield better functional results, specially where the patient is younger, highly active or where a type III injury does non reply to conservative management. For blazon 4 and Five surgical repair is highly recommended.
There are several surgical methods, simply the four nigh mutual surgical options are:
- Air-conditioning joint fixation using hook-plates
- coracoacromial ligament transfer
- coracoclavicular interval fixation
- a coracoclavicular ligament reconstruction.[22] [23]
Physical Therapy Management [edit | edit source]
Bourgeois - Types I and 2 [edit | edit source]
Initial handling should attach to the Law protocol including protection, optimal loading, water ice, compression, superlative and referral within the beginning 48 hours. A sling should be used to immobilise the shoulder along with keeping the shoulder in a elevated position when at remainder. Taping to help back up the joint can likewise be useful.
A sling can be in situ until the pain subsides. Return to normal activities is normally around 2-4 weeks for a blazon I injury, 4-6 weeks for a type II and 6-12 weeks for a type Iii[12]. For patients whose symptoms do not better within this frame, intra-articular steroid injections may be indicated [23]
There is, however, a lack of evidence regarding rehabilitation protocols. Reid et al developed a all-time practise guideline after a systematic review of electric current do[12]
Acute Phase [edit | edit source]
Range of motion (ROM): passive, active-assisted, active
- Glenohumeral Joint (GHJ): Internal rotation, external rotation, flex to tolerance : towel slides, pendular exercise



- Scapula: protraction, retraction, elevation, low
- Active-assisted exercise using a L bar for Internal and external rotation: GHJ xxx° to 45° abduction, 30° to 40° forward flexion:


Soft tissue: manage tightness
- Pectoralis minor stretch
- Posterior office of the GHJ: sleeper stretch
Isometric exercises: should be multi-bending, submaximal and subpainful
Closed Kinetic Chain: (no weight)
- hand supported in various planes and levels of elevation, control scapula position and progress to 90°
- elbow supported internal rotation/external rotation
- wall slides, scapula clock
- push-ups on wall


Recovery Phase [edit | edit source]
Avoid aggravation of the injury: case of exercises are demote printing, prone press-ups, shoulder press or dips. Proximal stability must exist reached earlier strength.
Range of movement: regain full range of motion of GHJ (including horizontal adduction), IR/ER at 90° abduction GHJ and capsular stretches.

Closed kinetic chain: increase the loads of previous closed kinetic chain exercises. Add active arm pinnacle and rotation.



Axial loaded active ROM (transition from closed kinetic chain to open kinetic chain (OKC)):
- wall slides with body and lower limb work
- wall slides in the scapular airplane
Kinetic chain:
- body and hip extension (scapular retraction) e.g. low row exercises

- trunk and hip flexion (scapular protraction) e.g. punches

- bilateral and unilateral pull with body rotations, e.grand. upper cuts
- Deltotrapezial complex work : exercises with cables, shrugs, abduction at various angles

Plyometric exercises (dynamic stretch shortening): medicine ball toss and grab, tubing plyometric exercises. Sport specific exercises: a two-manus overhead side to side throw for the overhead athlete.
[24]
Return to sport [edit | edit source]
Render to sport guideline:
- Grade I: ii-four weeks
- Form Two: 4-eight weeks
- Grade III: six-viii weeks
Post Operative - Types Five and Half dozen [edit | edit source]
Type Five and Half-dozen are considered to crave surgical repair and physical therapy may follow various mail surgical protocols.
Studies comparing the results of not-operative and surgical handling of type III Ac separations take shown that surgical interventions do not accept a substantial benefit. Bannister et al concluded that conservative management of type III injuries yielded a return to full shoulder kinematics more rapidly with less complications.[25] Conservative management should be considered equally the kickoff line of treatment for blazon III separations [26]
For type IV and Five injuries there is no evidence based literature recommending a specific treatment for these injuries. Surgery is the preferred treatment, but in that location has been a reported case of the successful use of transmission reductions, which converted the type IV to a type Two.[27]
Goals post surgery [edit | edit source]
- Control pain and swelling
- Protect the Air conditioning articulation repair
- Protect wound healing
- Brainstorm early shoulder move
Post surgical management [edit | edit source]
- Apply common cold packs to the operated shoulder to reduce pain and swelling.
- Remove the sling several times a day to gently movement the arm in a pendulum motion: lean forward and passively swing the arm.
- Use common cold to the shoulder for 20 minutes at a time every bit needed to reduce pain and swelling.
- Remove the sling several times a mean solar day: move the elbow wrist and hand. Lean over and do pendulum exercises for 3 to 5 minutes every 1 to 2 hours.
- To launder under the operated arm, bend over at the waist and let the arm passively come away from the torso. Information technology is condom to launder under the arm in this position. This is the same position every bit the pendulum exercise.
- Protocols on active motility and sling use will vary depending on the surgeon and the process done. Some will prescribe no active arm movements and the need for a sling for up to half dozen weeks. Others may allow sling use as needed and active movement immediately, for example up to 90 degrees in the first two weeks slowly progressing from there.
Post-operative rehabilitation and so follows similar guidelines every bit that for Type I and 2 injuries. Treatment consists initially of ROM exercises, followed past progressive strengthening. Rehabilitation needs to be followed through to total strength and mobility in order to avoid incidence of persistent pain and instability of the AC articulation.[28] [29]
Taping [edit | edit source]
[thirty]
References [edit | edit source]
- ↑ Codsi JM. The painful shoulder: when to inject and when to refer. Cleveland clinic periodical of medicine 2007; 74(seven): 473-482. (level of bear witness iv)
- ↑ Heijmans Eastward, Eekhof J; Neven AK. Acromioclaviculaire luxatie, huisarts & wetenschap, november 2022(level of show 5)
- ↑ Saccomanno MF. Acromioclavicular joint instability: beefcake, biomechanics and evaluation. Joints 2022; 2(2): 87–92.
- ↑ De Palma AF. Surgical anatomy of the acromioclavicular and sternoclavicular joints. Surg Clin North Am. 1963;43:1541–1550.
- ↑ Salter EG, Jr, Nasca RJ, Shelley BS. Anatomical observations on the acromioclavicular joint in supporting ligaments. Am J Sports Med 1987;fifteen(3):199-206.
- ↑ half-dozen.0 vi.1 6.2 6.3 Magee DJ, Zachazewski JE, Quillen WS. Pathology and Intervention in Musculoskeletal Rehabilitation.fckLRElsevier Health Sciences, 2008.
- ↑ Suezie Chiliad, Blank A, Strauss Eastward. Management of Type iii Acromioclavicular Articulation Dislocations Electric current Controversies. Bulletin of the Hospital for Articulation Diseases 2022; 72(1): 5360.
- ↑ Beim GM. Acromioclavicular joint injuries. Journal of Athletic Training 2000;35(3):261-267.
- ↑ Johansen JA, Grutter Pow, McFarland EG, Petersen SA. Acromioclavicular joint injuries: indications for treatment and handling options. J Shoulder Elbow Surg 2022;xx:70-82.
- ↑ Culp LB, Romani WA. Physical Therapist Examination, Evaluation, and Intervention Post-obit the Surgical Reconstruction of a Class Three Acromioclavicular Joint Separation. Journal of the American physical therapy association 2006; 86:857-869.
- ↑ 11.0 11.i Micheli LJ. Encyclopedia of Sports Medicine. London: SAGE Publications, 2022.
- ↑ 12.0 12.ane 12.2 12.3 12.four Reid D, Polson K, Johnson L, Acromioclavicular Joint Separations Grades I–Iii A Review of the Literature and Development of Best Practise Guidelines. Sports Med. 2022; 42(8): 681-696.
- ↑ Schneider MM, Balke M, Koenen P, Fröhlich M, Wafaisade A, Bouillon B, Banerjee K. Inter- and intraobserver reliability of the Rockwood nomenclature in acute acromioclavicular joint dislocations. Knee Surg Sports Traumatol Arthrosc. 2022; 24(7): 2192-half dozen.
- ↑ Nepola VJ, Newhouse EK, Recurrent shoulder dislocation. The iowa orthopaedic periodical 1993; 13: 97-106
- ↑ Robb AJ, Howitt S, Conservative direction of a type III acromioclavicular separation: a instance study and ten-year follow-up. Journal of Chiropractic Medicine 2022; 10: 261–271.
- ↑ xvi.0 16.1 sixteen.2 xvi.3 xvi.4 xvi.5 sixteen.6 Fraser-Moodie JA, Shortt NL, Robinson CM. Injuries to the acromioclavicular joint. J Bone Joint Surg. 2008 ;90-B: 697-707.
- ↑ 4. Johansen JA, Grutter PW, McFarland EG, Petersen SA. Acromioclavicular joint injuries: indications for treatment and treatment options. J Shoulder Elbow Surg. 2022;twenty p.S70-82
- ↑ 18.0 18.one Harris KD, Deyle GD, Gill NW, Howes RR. Transmission Physical Therapy for Injection-Confirmed Nonacute Acromioclavicular Joint Pain. Journal of orthopaedic & sports physical therapy 2022; 42(two): 66-80.
- ↑ 19.0 19.one Walton J, Mahajan S, Paxinos A, Marshall J, Bryant C, Shnier R, Quinn R, Murell GAC. Diagnostic Values of Tests for Acromioclavicular Articulation Pain. The Journal Of Bone & Joint Surgery 2004; 86-A (4): 807-812.
- ↑ Culp LB, Romani Westward. Physical Therapist Examination, Evaluation, and Intervention Post-obit the Surgical Reconstruction of a Grade III Acromioclavicular Articulation Separation. Periodical of the American physical therapy clan 2006; 86:857-869.
- ↑ nabil ebraheimExamination Of The AC Articulation - Everything You Need To Know - Dr. Nabil Ebraheim. Available from https://www.youtube.com/sentinel?v=daPnkXo03yM&t=1s
- ↑ Johansen JA, Grutter Pow, McFarland EG, Petersen SA. Acromioclavicular joint injuries: indications for treatment and treatment options. J Shoulder Elbow Surg. 2022;20: S70-82
- ↑ 23.0 23.1 Hootman JM. Acromioclavicular Dislocation: Bourgeois or Surgical Therapy. Athl Train. 2004; 39(1):10–eleven.
- ↑ Physio Fettle | Physio REHAB | Tim Keeley"Weight-lifter'southward shoulder" pain from an unstable AC joint | Feat. Tim Keeley | No. 27 | Physio REHAB. Available fromhttps://www.youtube.com/watch?five=aLj--YqCXhw&t=2s
- ↑ Bannister GC, Wallace WA, Stableforth PG, Hutson MA. The management of acute acromioclavicular dislocation. A randomised prospective controlled trial. Bone Joint Surg Br. 1989; 71(5): 848-850.
- ↑ Nissen CW, Chatterjee A. Type Three acromioclavicular separation: results of a recent survey on its management.Am J Orthop (Belle Mead NJ). 2007 Feb. 36(ii):89-93.
- ↑ Johansen JA, Grutter Prisoner of war, McFarland EG, Petersen SA. Acromioclavicular articulation injuries: indications for treatment and treatment options. J Shoulder Elbow Surg. 2022;twenty p.S70-82
- ↑ Johansen JA, Grutter PW, McFarland EG, Petersen SA. Acromioclavicular joint injuries: indications for handling and treatment options. J Shoulder Elbow Surg. 2022; twenty: S70-82
- ↑ Glick JM, Milburn LJ, Haggerty JF, Nishimoto D. Dislocated acromioclavicular articulation: follow-upwardly study of 35 unreduced acromioclavicular dislocations. Am J Sports Med 1977; 5: 264-70.
- ↑ KT Tape. KT Tape: Ac Joint. Bachelor from: https://www.youtube.com/sentinel?v=DJEhxOkg8Pg [last accessed 28/3/xv]

Source: https://www.physio-pedia.com/Acromioclavicular_Joint_Disorders
Posted by: cordovaworythe1986.blogspot.com
0 Response to "How To Repair An Ac Joint"
Post a Comment